Illness as trigger of T3 depletion
Science understands this process of T3 depletion as “non-thyroidal illness.” It has been called “non-thyroidal” because paradoxically, people with normal thyroid glands experience this deep, yet temporary hypothyroidism when they become very ill.
It is believed that during illness, the body protects itself by lowering its metabolic set-point. The most efficient way of doing this is to reduce the supply of the active thyroid hormone, T3, that is essential to raising metabolic rate.
The danger of Low T3
Research has proven, over and over, that if a person experiences “non-thyroidal illness,” they are at very high risk.
- The lower T3 drops, the higher the risk of DEATH and continued illness.
- Low T3 is a powerful predictor of poor outcome than any other indicator.
Therefore, researchers are now starting to consider Low T3 pathological, so much so that they are performing studies of therapeutic approaches to help patients with low T3 during various stages of the illness and recovery process.
Read more about the research on “Non-thyroidal illness” here
L-T4 monotherapy as trigger
Illness is not a prerequisite for Low-T3 syndrome.
According to the well-established theory of what triggers it, the body’s set-point does not have to lowered, T4 just has to be higher than the set-point.
Everyone has a DIO3 gene that makes D3 enzyme. Everyone’s DIO3 gene is sensitive to T4 levels above the body’s individual set-point.
The thyroid hormone set-point is different for each individual. Science has long ago proven that each healthy individual has a set-point for thyroid hormone levels that is 50% narrower than the statistical population reference range. One’s internal set-point for thyroid hormone cannot be predetermined by an external “reference range.”
L-T4 monotherapy causes a T3:T4 ratio that is significantly lower than healthy people. Because of this, a patient may require more T4 in bloodstream in order to have sufficient T3 hormone for normal physiological function. We already know that patients with the highest T4 levels often have extremely low T3 levels (very low T3:T4 ratios).
Therefore, some patients may be maintained at a L-T4 dosage that continually triggers T3 depletion.
Every day, their thyroid pill adds more T4, and every day, their body removes the slight “excess” T4 at the price of a T3 deficit.
If a thyroid patient gets sick, they can’t just turn down their natural thyroid production to prevent T4 “excess.” They depend on a static dosage of L-T4 medication. Their dosage can easily exceed a “set point” that becomes lower due to an illness.
But nobody is watching out for Low-T3 hypothyroidism in thyroid patients.
Why?
No Free T3 testing for you!
It’s not standard practice to measure thyroid patients’ Free T3 levels.
Current guidelines say to test only TSH, once a year, for the rest of your life on thyroid therapy.
The problem is — T3 depletion happens while TSH is maintained.
Yes, that is correct. TSH will not rise if only the active hormone, T3, drops.
Why?
If you are replacing a thyroid gland with a T4 pill every day, your dosage rigidly maintains T4. This maintains a TSH within the target range for L-T4 therapy — even if T3 drops. Hiding underneath that normal or suppressed TSH and a normal or high-normal T4 may be a T3 deficiency.
Only Free T3 testing can reveal Low T3 and low T3:T4 ratios in treated thyroid patients.
Recovery?
For a discussion of what we know about patients’ recovery from T3 depletion, see part 2:
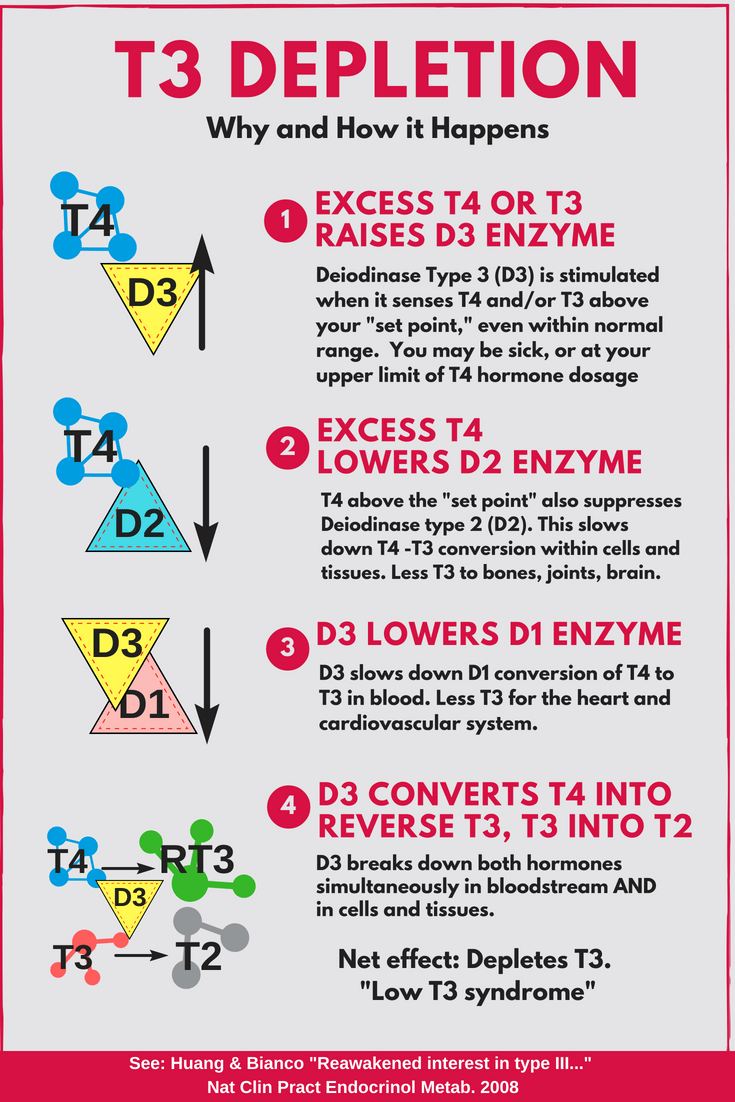
[…] But when people experience critical illness, their body’s set-point lowers and they experience T3 depletion. This is known as “non-thyroidal illness” or “low T3 syndrome” or “euthyroid sick syndrome.” The key player in this process is Deiodinase type 3, which is very sensitive to levels of thyroid hormone above the set-point, and causes a complex series of shifts in the body that lead to T3 depletion (as shown in the image). The lower the T3 level drops, the more the patient is likely to remain very sick, or die. Examine this process in more detail in our post on the GRAPHIC: T3 Depletion. […]
[…] For Part 1, see GRAPHIC: T3 Depletion […]
[…] GRAPHIC and discussion: T3 Depletion […]
[…] body has a safety mechanism to handle a short-term overdose of thyroid medication (see T3 depletion), but there is no safety mechanism to protect a thyroid patient from a […]
[…] Some T4 conversion difficulties are due to the inflexibility of thyroid hormone dosing, since patients can no longer flexibly adapt their thyroid gland’s secretion of T4. When a steady dose of T4 hormone is continually above a patient’s metabolic set-point, or if a patient’s illness reduces that set-point, the conversion rate will slow down even more, and the rate of T4 conversion into Reverse T3 increases, depleting T3 levels further. Unfortunately, if T3 drops too low, it is dangerous, and the body needs to increase T3 hormone to regain health during the recovery phase. (See “GRAPHIC and discussion: T3 Depletion“) […]
[…] Unfortunately, raising the L-T4 dosage will not necessarily raise a patient’s Free T3 level. In fact, raising L-T4 dose can lower T3. When a steady dose of T4 hormone is continually above a patient’s metabolic set-point, or when a patient’s chronic or critical illness reduces that set-point, their T4-T3 conversion rate will slow down even more, and the rate of T4 conversion into Reverse T3 increases, depleting T3 levels further. Unfortunately, if T3 drops too low in critical illness, it can endanger one’s life, and the body needs to increase T3 hormone to regain health during the recovery phase. (See “GRAPHIC and discussion: T3 Depletion“) […]
[…] our infographic and post that explains the big picture of “T3 depletion” in more […]
[…] leading to T3 depletion. See our infographic and post that explains the big picture of “T3 depletion” in more […]
[…] also upregulates the enzyme that inactivates both of the thyroid hormones, with a net result of T3 depletion that occurs simultaneously in the bloodstream and in peripheral tissues. This state will be […]
[…] GRAPHIC and discussion: T3 Depletion […]
[…] We don’t measure T2 outside of research, but the same enzyme that makes T4 into RT3 also steals our T3 by turning it into T2 at the same time. That’s why it leads to T3 depletion. […]
[…] disease diagnosis. They also falsely presume that such patients will all recover from their low FT3 (research shows no, they can and do often die or remain ill if FT3 is too low and stays too low). They also teach that in recovery from sick euthyroid syndrome, T3 levels are insignificant […]
[…] GRAPHIC and discussion: T3 Depletion […]
[…] GRAPHIC and discussion: T3 Depletion […]