 On April 8, 2018 The Canadian Society for Endocrinology and Metabolism (CSEM) made the happy announcement that they have made an edit to their prohibition of FT3 and FT4 testing in hypothyroidism.
On April 8, 2018 The Canadian Society for Endocrinology and Metabolism (CSEM) made the happy announcement that they have made an edit to their prohibition of FT3 and FT4 testing in hypothyroidism.
At first, patients were elated, hopeful, feeling like they were finally being heard! Maybe the Canadian Thyroid Foundation said something to open the eyes of endocrinologists.
Then we looked more closely.
This post shows that the edit is superficial, like changing the title of a book to create a better fit with the contents of that book.
The edit is expressed in these words:
“CSEM has modified recommendation #3 on the Endocrinology and
Metabolism list to clarify that patients should have access to additional testing, as required. The recommendation is now:Don’t use Free T4 or T3 to screen for hypothyroidism or to monitor and adjust levothyroxine (T4) dose in patients with known primary hypothyroidism, unless the patient has suspected or known pituitary or hypothalamic disease.”
WHAT REALLY CHANGED?
The phrase “unless the patient has suspected or known pituitary or hypothalamic disease” is not really a new update of their August 2017 toolkit.
The edit only adds words to the summary of the recommendation found on page 2 of their toolkit.
This reason for testing free thyroid hormones, “pituitary or hypothalamic disease,” was already discussed many times within the document.

The 2017 version of the Choosing Wisely toolkit “Less is More with T3 and T4” already acknowledged in many places that pituitary and hypothalamic hypothyroidism (also known as “central hypothyroidism” and “secondary hypothyroidism”) makes it necessary to test at least FT4 in addition to TSH
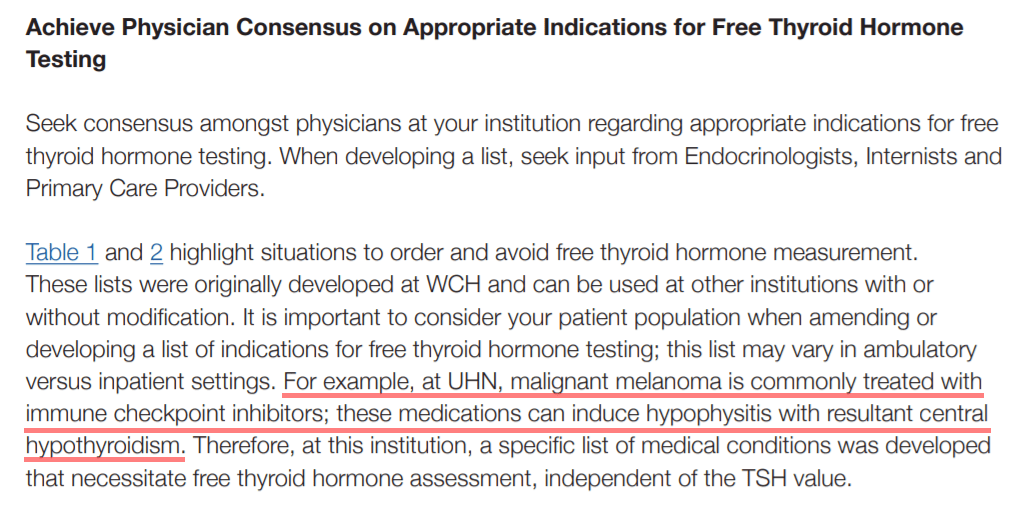
TABLE 1

The old toolkit already included central hypothyroidism (pituitary or hypothalamic diasease) in its recommended poster on page 22.

In the paragraphs of discussion, two situations were mentioned in which central hypothyroidism would allow additional testing, but only Free T4 testing. One was the suspicion of central hypothyroidism.

Another example given was drug-induced central hypothyroidism, in which “hypophysitis” is a condition involving inflammation of the pituitary gland:
As one can see, the edit is not a core change, but a decision to highlight one of the many reasons why a physician may wish to order FT4.
IS THIS EXCEPTION SIGNIFICANT?
Of course, the exception that central hypothyroidism ought not be diagnosed and managed by TSH is extremely significant to any person who has central (secondary) hypothyroidism.
But let’s look at what this exception means for the average hypothyroid patient on T4 monotherapy who has primary hypothyroidism (thyroid gland failure).
QUESTION: How rare is central hypothyroidism?
ANSWER: It is as rare as 1 in every 1000 patients with primary hypothyroidism. (Clemens, 2011; Beck-Beccoz et al, 2017)
However, experts debate whether central hypothyroidism is truly as rare as the statistics say.
The diagnosis and therapy of central hypothyroidism is challenging, especially in a system where laboratory reflex testing only measures Free T4 when TSH is below normal.
TSH may even be normal or high in some forms of central hypothyroidism (patients can have bioinactive TSH caused by hypothalamic tertiary dysfunction).
Cases of milder central hypothyroidism exist, as well as multiple types of drug-induced central hypothyroidism.
It creates a perpetual chicken and egg situation. You would need both the egg (Free T4 test) and the chicken (TSH test) before one can have a suspicion of hypothalamic failure, in the absence of other pituitary disorders.
Bottom line: It is truly not so easy for the average physician to “suspect” central hypothyroidism and know when to test Free T4. (Persani, 2012)
Therefore, the minor edit and the exception of central hypothyroidism is NOT a way of opening a door to dialogue with the majority hypothyroid patients, and it is NOT doing enough to help the patient who might have a milder form of central hypothyroidism.
See Part 2 of our response: CSEM attempts to dialogue with thyroid patients, April 8, 2019
REFERENCES
Beck-Peccoz, P., Rodari, G., Giavoli, C., & Lania, A. (2017). Central hypothyroidism – a neglected thyroid disorder. Nature Reviews. Endocrinology, 13(10), 588–598. https://doi.org/10.1038/nrendo.2017.47
Canadian Society of Endocrinology and Metabolism. (2019, April 8). CSEM Review and Response: Choosing Wisely Canada Recommendation #3: Testing and Management of Primary Hypothyroidism. Retrieved from http://www.endo-metab.ca/images/stories/pdf/csem-thyroid-testing-and-management-response-2019.pdf
Choosing Wisely Canada, Gilmour, J., & Mukerji, G. (2017, August). Less is more with T3 & T4: A toolkit for reducing free thyroid hormone testing. Version 1.0. Retrieved from https://choosingwiselycanada.org/wp-content/uploads/2017/09/CWC_T3T4_Toolkit_V1.pdf
Clemens, K., Payne, W., & Van Uum, S. H. M. (2011). Central hypothyroidism. Canadian Family Physician, 57(6), 677–680. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3114669/
Persani, L. (2012). Central Hypothyroidism: Pathogenic, Diagnostic, and Therapeutic Challenges. The Journal of Clinical Endocrinology & Metabolism, 97(9), 3068–3078. https://doi.org/10.1210/jc.2012-1616
Leave a public reply here, on our website.