 “T4 is converted into T3 at the cellular level in virtually all organs”
“T4 is converted into T3 at the cellular level in virtually all organs”
This is what Canada’s endocrinologists claim at the opening of their statement under their recommendation “Don’t use Free T4 or T3 to screen for hypothyroidism or to monitor and adjust levothyroxine (T4) dose in patients with known primary hypothyroidism.”
What does this statement so obviously omit? Disorders in thyroid hormone conversion.
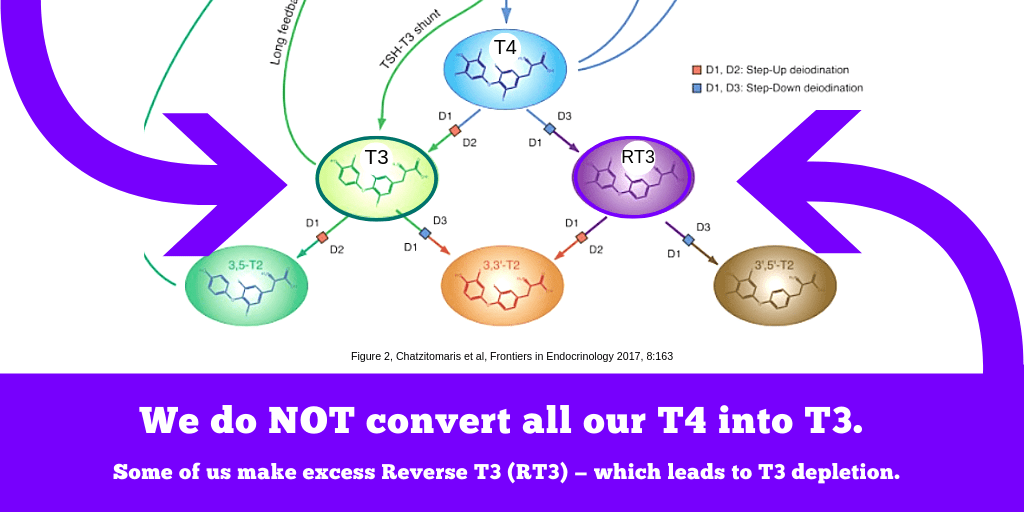
No, the human body does not merely convert T4 into T3.
Such a simplistic statement hides the truth that during T4 monotherapy, many patients experience lower T4 conversion to T3, and more T4 conversion into “Reverse T3” instead.
REVERSE T3
Conversion to Reverse T3 is not just a phenomenon that happens in illness. If you look at the teachings of thyroid biology, illness is simply not the only cause and trigger of thyroid hormone inactivation and excess Reverse T3.
The enzymes that create Reverse T3 are active in almost every tissue in our body, ready to spring to action whenever the slightest excess of T4 or T3 creates a need for thyroid hormone inactivation.
In the ill patient with a normal thyroid, T4 conversion to Reverse T3 happens because the body wants to lower the metabolism by diverting production of T3 to RT3 instead.
In the T4-treated thyroid patient, chronic excess RT3 happens because you continually resupply them with the same level of T4 hormone every day, which they might have difficulty converting into T3.
If T4 is even slightly higher than the body’s set point, every day a lot of T4 gets inactivated to Reverse T3, and every day this cycle repeats when you ingest more T4.
We don’t measure T2 outside of research, but the same enzyme that makes T4 into RT3 also steals our T3 by turning it into T2 at the same time. That’s why it leads to T3 depletion. (2)
OUR PERSONAL T4 TIPPING POINT
Even beyond bloodstream where T4 and T3 cannot be measured, thyroid scientists know that a mild excess of T4 that goes past a tipping point can drastically reduce T4-T3 conversion and enhance conversion to Reverse T3 instead, especially in the brain. (2, 3)
This may be why so many treated thyroid patients experience hypothyroid symptoms as cognitive decline and mood disturbances despite TSH being in normal range, if Free T4 is too high and T3 is too low — despite both hormones being within the statistical population reference range.
In other words, if you go past the tipping point, which is different for each individual and may be located in the upper-normal FT4 reference range, you can lose a lot of T4 into a bottomless pit of RT3 … and your FT3 can actually drop after an increased T4 dose.
THE FT3:T4 RATIO
But you don’t need to test Reverse T3 to see this happening.
The effects of excess conversion to Reverse T3 can usually be seen in a low fT3:T4 ratio in blood in a patient treated on standard T4 monotherapy.
In general, thyroid patients’ fT3:T4 ratio is significantly lower than normal people with healthy thyroid glands. (4, 5)
Specifically, the fT3:T4 ratio in healthy patients with normal thyroid glands is usually maintained in a tight range around 0.31 to 0.33 pmol/L, but in T4-treated patients the average is 0.23 to 0.24 pmol/L. (5)
What these averages obscure is the narrow control of FT3 levels in healthy patients and the wide variation in FT3:FT4 between individuals on thyroid therapy.
Thyroid patients can suffer an incredibly low T3 below reference range.
In fact, some Canadian thyroid patients whom we know personally have suffered a ratio as low as 0.14, with a high Reverse T3 at the same time, over the long term.
What makes the fT3:T4 ratio drop so low in some treated thyroid patients? Two factors:
1) a person’s lack of thyroid tissue, and
2) some individuals are less able to convert T4 into T3. (4)
Now that we know how different treated patients are from healthy patients, let’s return to the Endocrinology association’s further dismissal of Free T3 and Free T4 measurement in patients treated with levothyroxine.
3 MORE PROBLEMS IN THEIR NEXT CLAIM …
See part 2: The pituitary response is abnormal. Stop TSH worship.
REFERENCES
IMAGE: Chatzitomaris, A., Hoermann, R., Midgley, J. E., Hering, S., Urban, A., Dietrich, B., … Dietrich, J. W. (2017). Thyroid Allostasis–Adaptive Responses of Thyrotropic Feedback Control to Conditions of Strain, Stress, and Developmental Programming. Frontiers in Endocrinology, 8. https://doi.org/10.3389/fendo.2017.00163
(1) #3 in Endocrinology and Metabolism: https://choosingwiselycanada.org/endocrinology-and-metabolism/
(2) Gereben, B., Zeöld, A., Dentice, M., Salvatore, D., & Bianco, A. C. (2008). Activation and inactivation of thyroid hormone by deiodinases: local action with general consequences. Cellular and Molecular Life Sciences: CMLS, 65(4), 570–590. https://doi.org/10.1007/s00018-007-7396-0
(3) Werneck de Castro, J. P., Fonseca, T. L., Ueta, C. B., & McAninch, E. A. (2015). Differences in hypothalamic type 2 deiodinase ubiquitination explain localized sensitivity to thyroxine. Journal of Clinical Investigation, 125(2), 769–781. https://doi.org/10.1172/JCI77588
(4) Midgley, J. E. M., Larisch, R., Dietrich, J. W., & Hoermann, R. (2015). Variation in the biochemical response to l-thyroxine therapy and relationship with peripheral thyroid hormone conversion efficiency. Endocrine Connections, 4(4), 196–205. https://doi.org/10.1530/EC-15-0056
(5) Gullo, D., Latina, A., Frasca, F., Le Moli, R., Pellegriti, G., & Vigneri, R. (2011). Levothyroxine Monotherapy Cannot Guarantee Euthyroidism in All Athyreotic Patients. PLoS ONE, 6(8). https://doi.org/10.1371/journal.pone.0022552
Leave a public reply here, on our website.